20 Oct Why you shouldn’t always stretch
WHY YOU SHOULDN’T ALWAYS STRETCH?
“After an injury tissues heal, but muscles learn, they readily develop habits of guarding that outlast the injury” Janet Travell

Have you ever had a muscle group that was perpetually tight and despite all your efforts at stretching, they remain stiff? Muscles do get tight when overworked, say after a long run for instance. But what many of my patients think are chronically tight muscles, are often chronically “guarded” muscles.
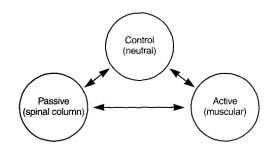
The figure above is taken from Panjabi and White Biomechanics of the Spine. It depicts the integration between our nervous system, spinal column and muscular system.
The joints of the human body have nerve receptors called “mechanoreceptors” and “proprioceptors”. These receptors signal the brain telling the brain transmitting information about compression, tension, and position of the joints. When motion could potentially cause damage, a “red light” signal is sent to the brain to prevent movement and further damage. Our pain receptors, called “nociceptors” are one source of red lights. Red light signals the brain to reduce/ protect certain ranges of motion and slow down speed of contraction and reduce force production down in certain muscles. Some muscles can have increased “gain” or more input to cause the muscle to guard and protect movement. This is often the case with so perceived “tight hamstrings”. For many of my patients that lack adequate core stability, the hamstring tightness they perceive is actually guarding mechanism driven by the brain and feedback from the joints in order to prevent injury. In my clinic, chronically tight hamstring is most often considered muscle guarding until proven otherwise. Very often by increasing core strength we can get the hamstring muscles to unwind.
Spasm and guarding are always protective and should be an alert that something is amiss. Therefore, a resounding “NO”! we should not always stretch a tight muscle.
UNDERSTANDING PROTECTIVE TENSION
Protective tension is a contraction of muscles to prevent excess load onto tissues. It serves you by limiting your range of motion to protect an injured or unstable joint. Protective tension can alter biomechanics to create compensated movement to avoid loading injured areas. When we take these muscles to tension, what we often feel is a stretch, perhaps pain or even nothing at all. Most often patients are unaware that the tension they may or may not feel exists to guard and protect them from further injury.
Contrast that with stretching a tissue at end range and feeling a slight stretch sensation. The feeling is often exactly the same with guarding, although the range of motion may be much more limited in the setting of protective tension.
TIGHT DOES NOT EQUAL STRETCH!!! THINK ABOUT WHAT IS HAPPENING BEFORE APPLYING TREATMENT, ESPECIALLY STRETCHING.
Nerves do not like to be stretched. Think about pulling on both ends of a cooked spaghetti noodle. It just breaks. While nerves are resilient and protected for the most part, when they are stretched their blood supply gets cut off. Blood vessels coil around our nerves to allow for physiological movements of the nerve and provide oxygen. As a nerve is stretched beyond 15 % of its resting length, this blood flow is compromised and the sensation that is experienced can be likened to a burning type sensation, or severe stretch. Since peripheral nerves easily become entrapped throughout the body, whereby they essentially become glued down to tight fascia, nerves are often succumb to overstretching due to restricted fascial movement. This often results in paresthesias or abnormal, uncomfortable nerve sensations like pain, burning, pins and needles and numbness.
Most of my patients use foam rollers and stretch. Although many of them self report they don’t feel like they stretch enough. If foam rolling, yoga and some basic mobility are not resolving your tight spots, then there is likely more than meets the eye. Get it looked at.
References: Panjbai and White. Clinical Biomechanics of the Spine. Lippincott