05 Oct Debunking Shoulder Pain in the Overhead Athlete


One of the most common syndromes that plague athletes and fitness enthusiasts is shoulder pain. Most commonly the pain occurs during or immediately following exercise and is located along the front of the shoulder and slightly less common in the back of the shoulder. Often times there will be no pain during exercise, but may occur with daily activities, like reaching overhead or behind the back.
In this blog I will address the causes of shoulder pain in the overhead athlete. Keep in mind that shoulder pain is not unique to Overhand Athletes (think baseball, volleyball, swimming, tennis) but is common to many in sport and fitness. Whether you are a CossFitter, a runner, an Orange Theory Fitness addict or just a recreational athlete, shoulder problems plague many of us. In fact, shoulder injuries comprise about half of all the CrossFit and strength training related injuries we see in our practice.
Disclaimer:
Paging Dr. Google…much of the information that is available on the internet, while in part helpful and correct, is often not comprehensive and can be misleading when not placed in the right context. Many of the quick fix “Do this Exercise” posts to fix your shoulder pain leave much expertise to be had, leaving the reader/athlete with an incomplete explanation of the big picture and the true causative factors which are all too often multi-factorial in nature.
I. Defining the Problem: It all starts with an accurate diagnosis.
With any musculoskeletal pain syndrome lasting longer than 2 weeks, getting an accurate diagnoses by a well-trained sports medicine physician is paramount. The spectrum of most shoulder injuries covers basic functional shoulder impingement, biceps and rotator cuff tendonitis to the more severe partial and full thickness rotator cuff tears and labral tears.

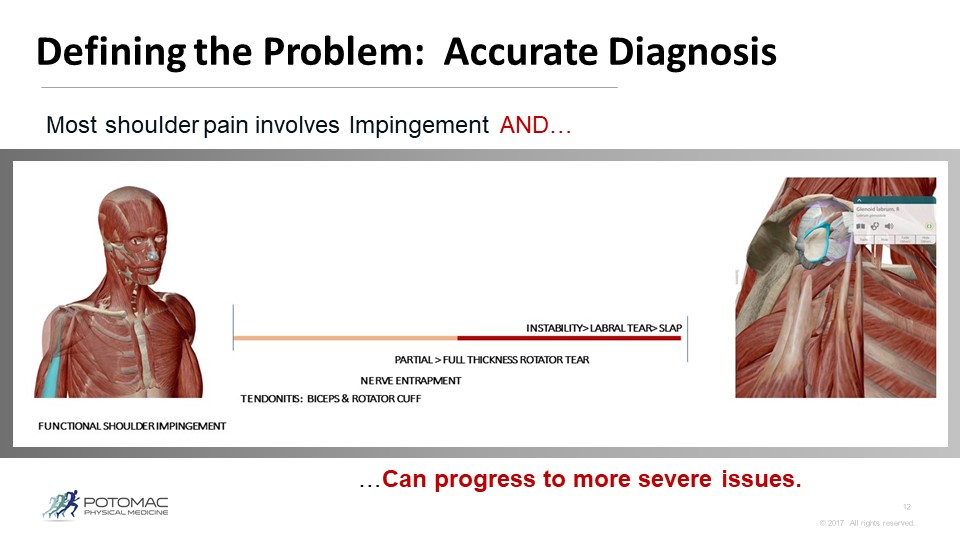
PICTURES COURTESY OF THE HUMAN VISIBLE BODY APP
The big key here is that most shoulder injuries are the result of repetitive motion injury over time, and not the result of acute sport setting trauma. Excluding falls on outstretched arm, traumatic dislocations or abrupt tears due to trauma, the remaining 90 % or more of shoulder problems occur over a more lengthy period of time. When gradual shoulder pain surfaces, or even sharp pain that occurs abruptly, you must respect the process. Evaluate your training volume. When was the last time you took a deload week to recover? What are your recovery practices? Many factors can lead to injury. The key to prevention is a good mobility practice to ensure you move properly. This requires consistent self care exercises as well as performance care from a sports doc, focused on physical medicine in which you are receiving manual body work in the form of joint and fascial manipulation. These practices are implemented by the pros to prevent injury and optimize performance. Good habits and practices can help mitigate the stresses of training and the cumulative repetitive microtrauma in the body tissues and joints.
In part II we will deep dive into biomechanics of shoulder movement. In Part III we will discuss some recovery techniques you can implement as well as explore the best evaluation & treatment options for getting a shoulder injury properly diagnosed and resolved quickly, and without surgery.
Want a preview for Part II? Keep Reading
Mobility/Stability Motor Control of the Shoulder Complex
Stability is often posited as the key to resolving shoulder pain, and while it is very important, it is not the end all be all. Focusing only on stability is a narrow aperture that causes several vital factors to be missed…
The soft tissues get tight overtime and actually glue together, resulting in restricted movement…Here are some helpful self care practices to help stay in front of this issue.

A Note on Mobility
Many athletes today use foam rollers, lacrosse balls and super bands to mobilize stiffness in the soft tissues. If consistent attempts to release the latissimus and posterior rotator cuff with foam roller / lacrosse ball are ineffective, this may be a telltale sign of more serious pathology in the GH joint, namely instability due to a rotator cuff tear or a labral tear. This recurring tightness is guarding tension and is protective in nature. Meaning, the instability must be addressed in order for these tissues to be successfully released.

Learn more about Active Release Techniques, a fast and effective treatment for soft tissue injuries.