01 Aug SHRUGGING OFF SHOULDER PAIN
by Dr. Matt Fontaine
This article will expand on topics we covered in our “SHRUGGING OFF SHOULDER PAIN” clinic as part of our 4- part Injury Prevention and Performance Clinic Series in partnership with Trident CrossFit.
Patients with injury and pain who seek medical care deserve:
- An accurate Diagnosis
- A well devised treatment plan
- Set goals and predictable outcomes from treatment
Shoulder Pain 101: Common Problems
Shoulder pain affects hundreds of thousands of athletes and active individuals. Shoulder pain can be the result of simple impingement of the shoulder but can also be due to more serious causes like partial and full thickness rotator cuff tears and labral tears (most commonly, SLAP tears). Partial tears involve less than 50 % of the thickness of the tendon while full thickness tears are a complete rupture through the tendon and muscle.
The biggest challenge facing these athletes is the lack of a specific diagnosis. They are often diagnosed with:
- Shoulder Impingement
- Biceps tendonitis
- Bursitis
- Rotator cuff Injury, including tendonitis
These terms are simply to vague to best guide our treatment plan.
So, what do these terms actually tell us? Where exactly is the problem?
Is there an actual biomechanical problem with the shoulder movement? Is there a repetitive motion injury? For many, these questions remain unanswered. The most common and most commonly undiagnosed problem and easily treated dysfunction is the myofascial adhesion, scar tissue within muscles that restricts movement.
A specific diagnosis of adhesion and joint movement requires a hands on physical examination to include palpation and assessment of the movement of the neck (cervical spine), upper back (thoracic spine), shoulder girdle (scapula, scapulothoracic, acromioclavicular and sternoclavicular articulations) as well as the ball and socket of the shoulder, the glenohumeral joint.
Often times MRI or MR Arthrogram is needed to evaluate for a rotator cuff tendon tear, biceps tendon tear or SLAP tear.
For many patients, they see their primary care doctor and get a referral for physical therapy. Quite often, without ever receiving a specific diagnosis. Often times they will see an orthopedic who may order a simple X-Ray which is often read as normal. X-Rays are bone studies and do not properly evaluate soft tissues like muscles, tendons, fascia, ligaments and nerves.
Common Shoulder Symptoms
- Pain with overhead movement
- Painful arc between 90 and 120 degrees Abduction (raising arm out to the side)
- Posterior or anterior shoulder pain during bench press
- Pain with external rotation of the shoulder
- Clicking or pinching
- Pain behind the shoulder blade
- Sharp anterior shoulder pain
- Burning, numbness or tingling
- Numbness or tingling into the upper arm, forearm or hand, especially at night
Two of the Most Common Diagnosed Shoulder Injuries
- Biceps tendonitis (umbrella term, often over-diagnosed)
- Shoulder impingement
Both of these condition are too general. They do not address movement patterns, areas of adhesion (glued down muscle and fascia, nerve entrapments), nor specific anatomical structures that are injured.
Defining Shoulder Impingement
Shoulder impingement is typically classified as primary Outlet impingement or Non-outlet impingement. Outlet impingement refers to structures are the periphery of the glenohumeral joint, most notably the undersurface of the acromian process (red arrow below), where we can see thickening of the bursa and even bursal side partial and full thickness tears.

Non-Outlet impingement is typically due to instability, where the ball slides around loosely in the socket, which can damage the labral cartilage, resulting in SLAP tears. Non-outlet impingement typically affects the anatomical structures deep within the joint (green arrow above).

So What Does the Rotator Cuff Actually Do?
Though many refer to this as the rotator “CUP”, the tendons of the four rotator cuff muscles actually attach and blend into the capsule of the shoulder (think shrink wrap for joints) to form a compressive “cuff” surrounding the entire ball and socket joint.The primary role of the rotator cuff is to maintain the axis of rotation of the ball and socket joint throughout a full range of motion. Simply said, the rotator cuff muscles (supraspinatus, infraspinatus, subscapularis, teres minor) work synergistically to compress the ball (head of humerus) into the socket (glenoid of the scapula).
These pictures below show the normal rolling and sliding of the ball in the socket of the shoulder.
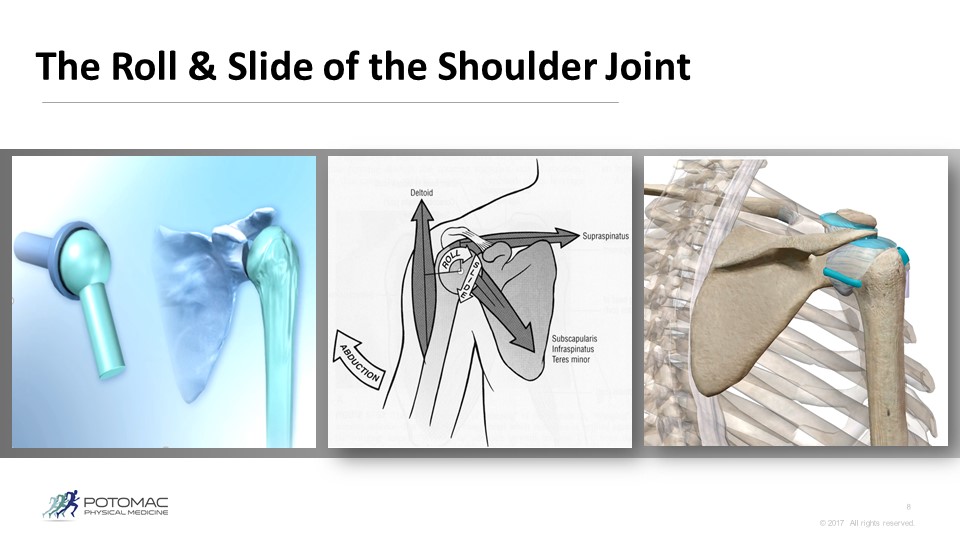
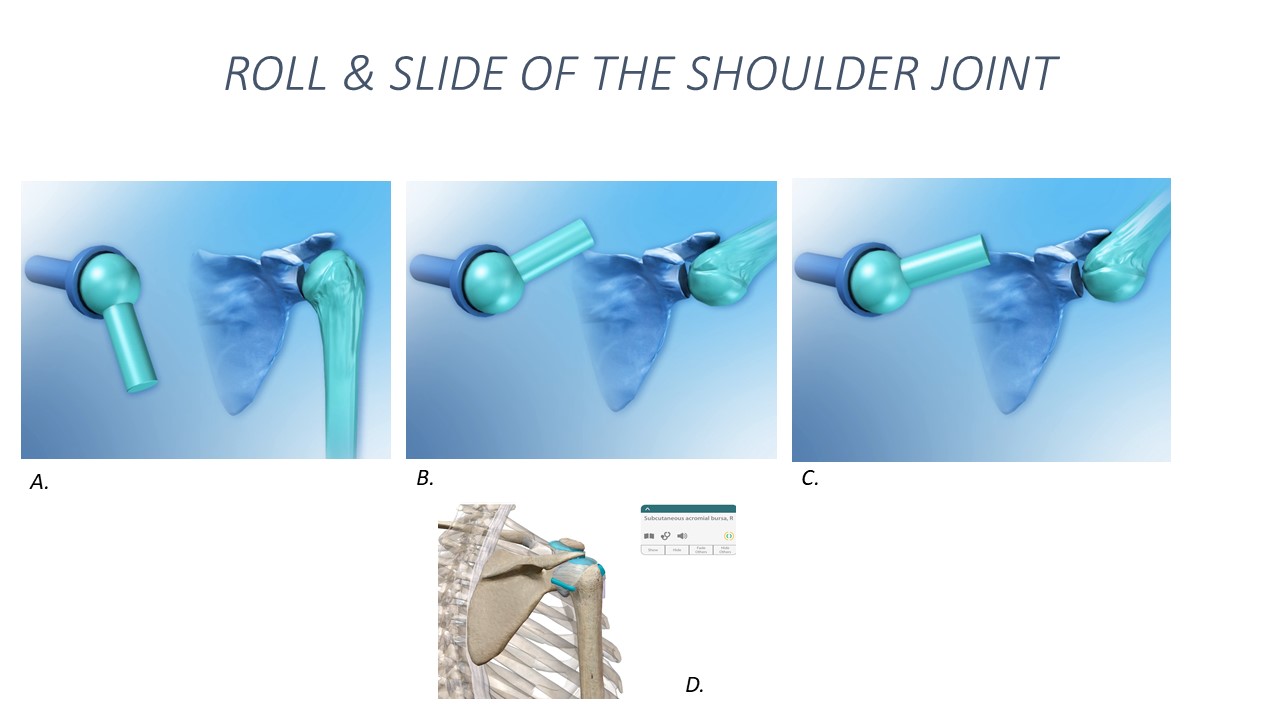

Photo above courtesy of Visiblebody App

The above diagrams show the different vectors of pull imparted on the joint by the rotator cuff muscles, which act during active range of motion to keep the shoulder in the socket.

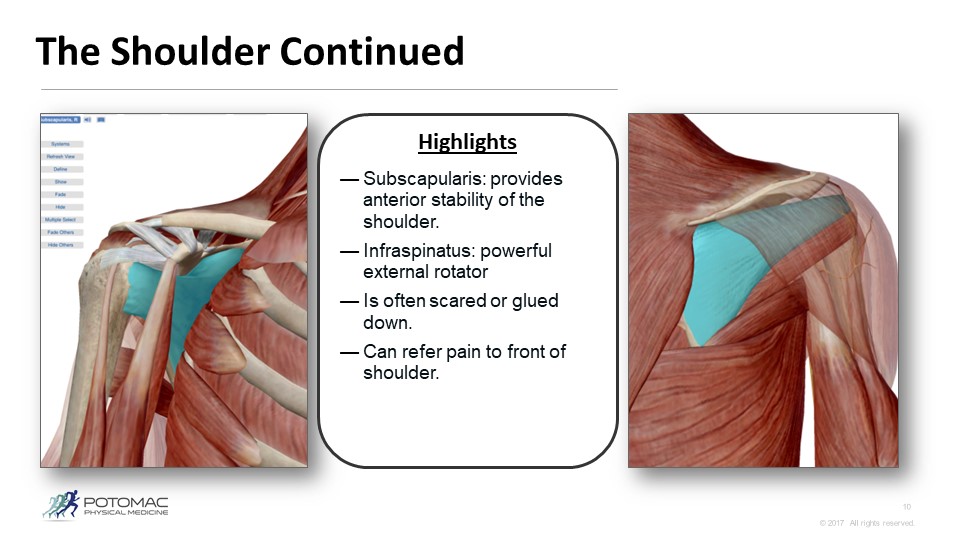
Pictures above are courtesy of the VisibleBody app.
Left: Front side of the shoulder, showing the Subscapularis (highlighted in blue)
Right: Back side of the shoulder, showing the Infraspinatus (highlighted in blue)

The above diagrams show to very important muscles of the rotator cuff, which act during active range of motion to keep the shoulder in the socket. The subscapularis (highlighted in blue in the left picture below) the biggest of the rotator cuff muscles sits in front of the shoulder blade, is largely responsible for preventing the ball of the shoulder from migrating forward. When this muscle gets injured and “glued down” it becomes weak, allowing the shoulder to shift forward in the socket and generating tremendous strain on the biceps tendon and anterior labral cartilage of the shoulder. The result is often tendonitis, impingement, and worse, labral tear.
The muscles of the rotator cuff can become tight over time and glued down due to repetitive motion. These muscles then become weak and can refer pain to the front and back of the shoulder. When the rotator cuff muscles become glued down, they no longer work optimally during shoulder motion. This can lead to impingement, biceps tendonitis, bursitis, and even rotator cuff tear and SLAP tears.

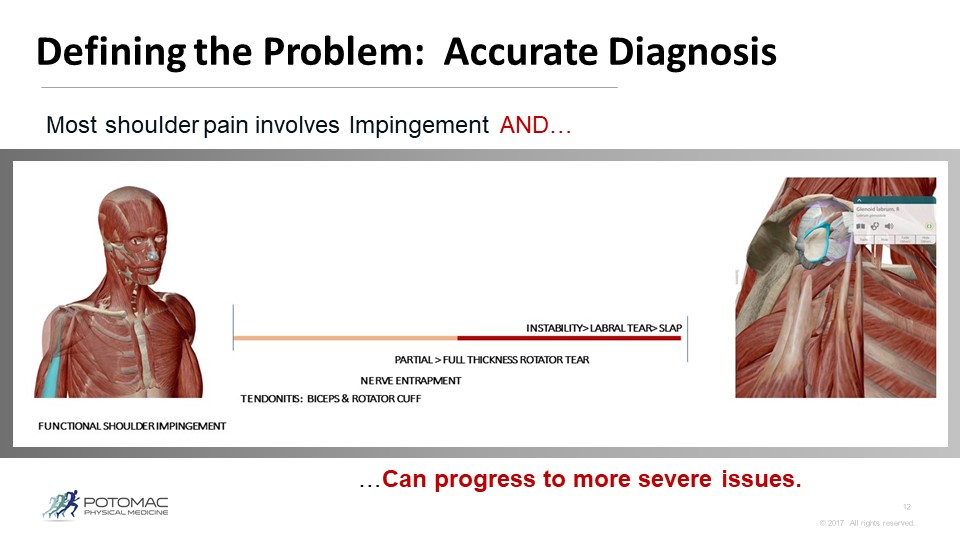
Shoulder Pain Covers a Wide Spectrum of Injuries
The picture below shows how a typical non-traumatic repetitive motion injury can progress over a wide range of possible causes. From simple impingement and biceps tendonitis, progressing to more severe rotator cuff tears and labral tears.

Key Take Aways
- PAIN ALWAYS FOLLOWS DYSFUNCTION> Shoulder pain lasting longer than 2 weeks should be evaluated by a physician. Find a good sports doc.
- Most pain is the result of repetitive motion injury which results in glued down muscles, fascia, tendons, shoulder joint capsule and nerves.
- Most cases of shoulder pain are due in part to poor positioning of the shoulder blade, known as an anteriorly tilted shoulder blade which tips forward and causes the shoulder blade to wing off of the rib cage and upper back.
- Work stability into your strength program> Cross Over Symmetry and kettlebell work can help. Kettlebell arm bar and bottom up kettlebell walking or lunges and Turkish Get Ups all require good stability of the shoulder girdle.
- Commonly prescribed “Y, T and W” exercises are not a catch all for stability.
What to do
Here are some tips on mobility drills to help improve with shoulder movement. Remember, mobility is critical, but so is stability.